OA Knee FAQs
OA Knee FAQs
article written by doctors of Asia Medical Specialists
(Last updated on: Oct 13th 2020)
What is osteoarthritis?
What causes osteoarthritis?
- Heredity - Slight joint defects or double-jointedness and genetic defects may contribute to the development of osteoarthritis.
- Obesity - Excessive weight can put undue stress on such joints as the knees over time.
- Injury - Significant injury to a joint, such as an anterior cruciate ligament (ACL) or meniscal tear, can later result in osteoarthritis.
- Overuse - Injury may also result from repeated overuse or misuse over a period of time. However, in people with normal knees, studies have shown that in former marathon runners, knee osteoarthritis is rare. Instead, the risk of hip osteoarthritis is higher than control subjects, though the reason is unknown [1].
What are the symptoms of osteoarthritis?
- joint pain
- joint stiffness, especially after sleeping or inactivity
- limited joint movement as the disease progresses
- grating of joints when moved (in more advanced stages of osteoarthritis) as the cartilage wears away
- locking
How is osteoarthritis diagnosed?
- X-ray – narrowing of the joint space as the cartilage thins, followed by thickening of the bone underneath the cartilage adjacent the joint (subchondral sclerosis), and then bone spurs (osteophytes) and finally cysts. (Fig. 1)
- MRI – can demonstrate pre-X-ray changes including localised cartilage damage or thinning, swelling (oedema) inside the bone, meniscus tears and small bone spurs.
- Blood tests – to rule out other causes of arthritis e.g. rheumatoid arthritis & gout.
- Joint aspiration - involves removal of any fluid from the joint to exclude infection or gout as possible causes.
Treatment for osteoarthritis
- your age, overall health, and medical history
- extent of the condition
- your tolerance for specific medications, procedures, and therapies
- expectation for the course of the condition
- your opinion or preference
Treatment may include:
Education
Reduce impact
- soft soled shoes
- activity modification
Exercise
• We suggest patients with symptomatic OA knee to participate in low impact aerobic exercises and incorporate
activity modifications into their lifestyle (e.g. walking and cycling instead of running) [2,3].
• Quadriceps strengthening is also effective for pain-relief and improves function [4].
Weight reduction
Patients with OA knee, who are overweight (Body Mass Index >25), are encouraged to lose a minimum of 5% of body weight and maintain their weight at a lower level with an appropriate dietary modification and exercise [2,3].
It has significant effects on pain and function, and health benefits extend beyond of the knee.
Omega-3 diet
A high Omega-3 low Omega-6 diet has a number of potential benefits including on the cardiovascular and immune systems, reduces macular degeneration in the eye and has anti-tumour effects.
Its role in musculoskeletal system is not fully understood, but recent research suggests there is anti-inflammatory activity, which may translate into clinical effects [5]. For example, there is evidence that rheumatoid arthritis patients taking omega-3 from sources such as fish have reduced pain compared to those receiving standard non-steroidal antiinflammatory drugs [6].
Physical and occupational therapy
Physical therapy may help to reduce joint pain and improve joint flexibility when performing daily activities, and reduce joint strain.
Unloader braces
Unloader braces are for people with arthritis on one side of the knee joint – either the inside or outside. The braces are intended to shift some of the stress away from the arthritic portion of the knee and onto the good part of the knee and thus provide pain relief (Fig.2).
Fig. 2 Unloader knee braces – the arrows represent the force applied by the braces to the knees to shift the load. |
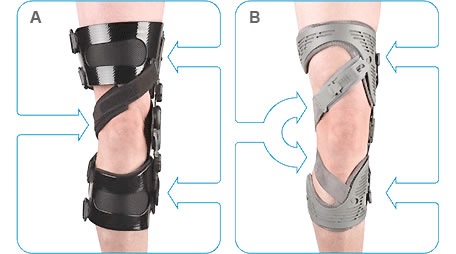
Unfortunately these braces are not very helpful for most people. A systematic review 7 concluded that there is only limited evidence for the effectiveness with no evidence for improvement in pain at 6 or 12 months. The small effects seen are not clinically important and not statistically significant [7].
Medication
Medication for specific symptoms may include pain killers and anti-inflammatory drugs. Commonly used agents are acetaminophen/paracetamol (Tylenol/Panadol), non-selective non-steroidal anti-inflammatory drugs e.g. ibuprofen (Brufen, Nurofen, Advil) or diclofenac (Voltaren) and selective cyclo-oxygenase-2 inhibitors, which are safer than non-selective anti-inflammatories e.g. etoricoxib.
Glucosamine & Chondroitin
These are ingredients of glycosaminoglycan, a major component of cartilage. They are beneficial in cartilage degeneration and treat osteoarthritis via many mechanisms [8,9,10,11]. Generally they are safe, with minimal side effects. They are food supplements, not drugs. They may slow down the progress of arthritis. They may provide pain relief similar to that of painkillers. The pain relieving effect begins after 2-3 weeks of taking glucosamine.
Intra-articular injection of steroid
Intra-articular steroid is effective for short-term pain relief. It acts through its anti-inflammatory action. The injection is a minor procedure performed in the office, requiring no anaesthesia. It is often very helpful in settling down an acutely painful knee, but it does not have any long-term benefit to the knee and multiple injections are probably damaging to the cartilage [12].
Viscosupplementation
Viscosupplements are liquids mimicking normal joint fluid. Injection of viscosupplements is a minor procedure performed in the office, requiring no anaesthesia. Generally it shows positive effects on knee pain and function [13]. The most commonly used viscosupplement is hyaluronic acid, which is a component of joint fluid.
Joint surgery
Surgery may be necessary to repair or replace a severely damaged joint. The options include: knee arthroscopy; chondroplasty; osteotomy; and partial or total knee replacement.
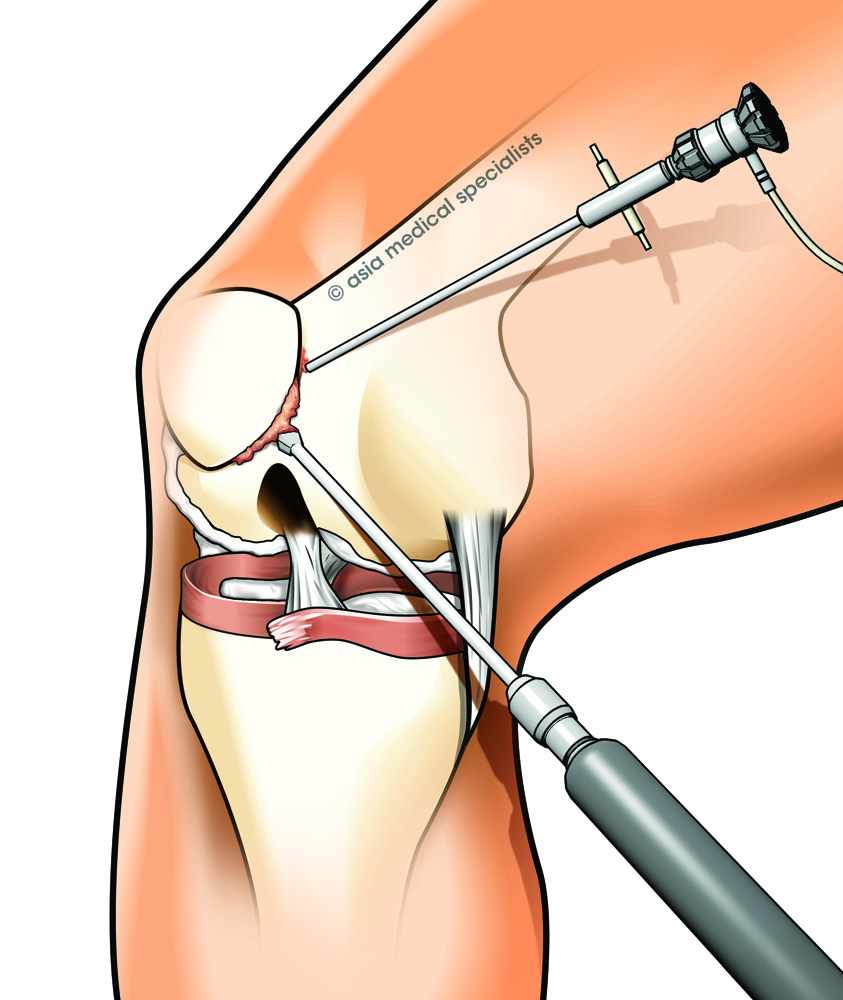
Arthroscopy
Arthroscopy (also known as 'keyhole surgery') is a common and simple procedure, in which the joint is viewed using a small camera (Fig. 3). It is an excellent option when there is a mechanical problem such as catching or locking suggestive of a loose body or torn meniscus. Usually it is done in the hospital as a day procedure and one can return to office work in a few days.
Fig. 3 Knee arthroscopy |
High tibial osteotomy or Unicompartmental Knee Replacement
If only one part of the knee is worn out, there is a choice of either high-tibial osteotomy (HTO) or unicompartmental knee replacement (UKR).
HTO
In patients with slightly bowed legs and arthritis mainly of the inside half of the knee, the angle of the shin bone can be changed to shift the stress onto the outer half of the knee that is not so worn out (Fig. 4). This is particularly helpful in patients too young to be optimal candidates for knee replacement.
Fig. 4 X-ray of HTO – the line represents the weight bearing axis, which is shifted by the HTO. |
Fig. 5 HTO fixed with locking plate. |

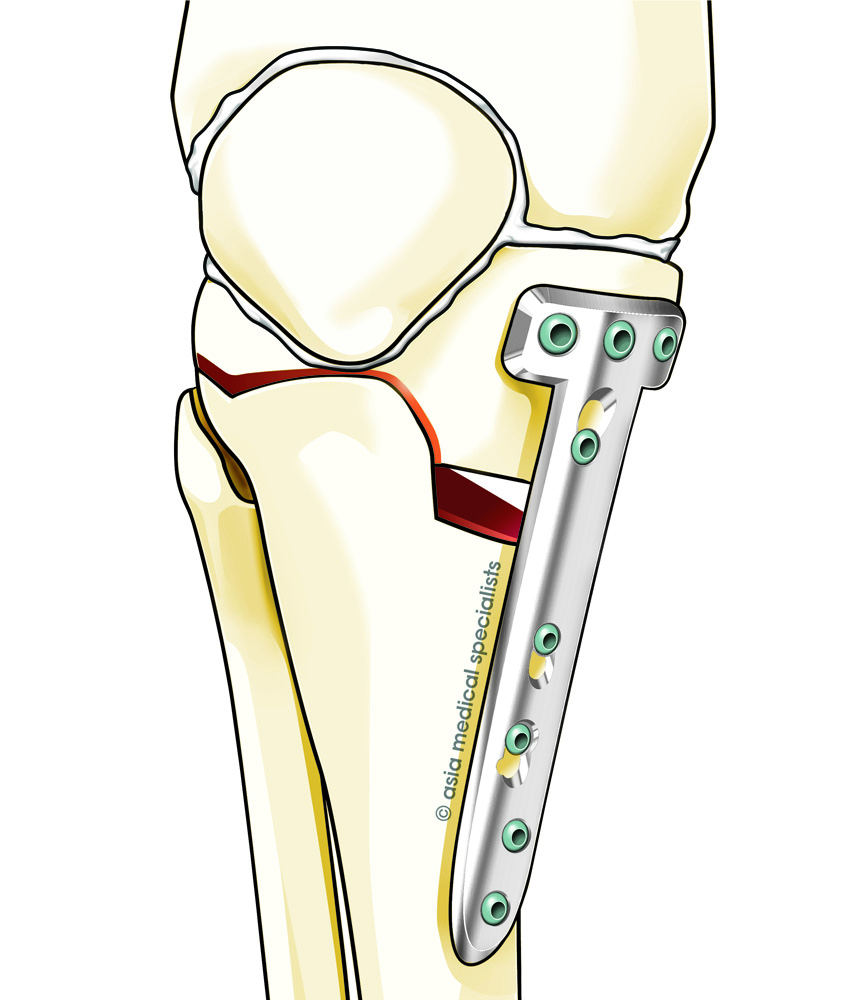
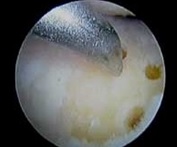
The procedure involves cutting ('osteotomy') at the upper shin bone and fixing it in a new position with a plate and screws (Fig. 5). Often an arthroscopic microfracture to regenerate new joint cartilage (fibrocartilage or scar tissue, not articular cartilage) is performed as an accessory procedure (Fig. 6 & 7).
Fig. 6 Arthroscopic findings of advanced knee osteoarthritis. Yellow coloured bone is seen where the cartilage is missing. |
Fig. 7 Arthroscopic microfracture chondroplasty – small holes are made in the bone to cause bleeding and healing with scar tissue (fibrocartilage). |
One will need to use crutches for 6 - 8 weeks until the bone heals. Usually it takes a few months for the osteotomy to heal fully and for regeneration of cartilage. HTO has a slower recovery than UKR (see below) but does not 'wear out' in quite the same way as an artificial joint, so is a good choice for younger more active individuals.
Around 90% of patients will have significant improvement for about 5 years, but it declines to only about 65% by 10 years [16,17,18,19,20]. As the arthritis progresses, and the pain returns, total knee replacement may be needed.
UKR
Unlike a total knee replacement, this less invasive knee procedure replaces only the most damaged part of the knee (Fig. 8). Recently it has been done through a smaller 'minimally invasive' incision, allowing the knee to recover faster. Most patients are walking with a cane in just a few days and are usually able to return to normal activities within a few weeks. UKRs offer excellent function, though not quite as good as a normal knee, and one should reduce impact and distance running to slow down the wear on the UKR.
Studies showed that in middle-aged patients with UKR, the ten-year survival rate of implants is around 80% [21,22]. If the pain recurs, total knee replacement is advised.
Fig. 8 X-Rays of UKR |
Fig. 9 TKR |

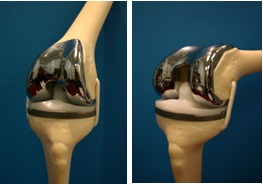
Total Knee Replacement
Total Knee Replacement (TKR) is for advanced arthritis. It replaces the surfaces of the entire joint (Fig. 9). One is required to stay in hospital for several days. Usually one walks with crutches the next day and with a stick after about 2 weeks.
A large study showed 92% total knee replacements last more than 15 years [23]. They last longer if you are not overweight and do not do hard physical work or play sports that excessively stress the joint. If you are older than 60, the artificial joint will probability last the rest of your life. If the TKR wears out, one will require a revision TKR – removing the original TKR and replacing it with a new one.
References
1. Is competitive running associated with osteoarthritis of hip or the knee? Schmitt H, Rohs C, Schneider S, Clarius M. Stiftung Orthopädische Universitätsklinik, Schlierbacher Landstrasse 200a, 69118 Heidelberg.
2. Zhang W., Moskowitz R.W., Nuki M.B. et al. OARSI recommendations for the management of hip and knee osteoarthritis, Part I: critical appraisal of existing treatment guidelines and systemic review of current research evidence. Osteoarthritis Cartilage 2007 June 16; 15:981-1000.
3. Zhang W., Moskowitz R.W., Nuki M.B. et al. OARSI recommendations for the management of hip and knee osteoarthritis, Part II: OARSI evidencebased, expert consensus guidelines. Osteoarthritis Cartilage 2007 December 20; 16:137-62.
4. Roddy E, Zhang W, Doherty M. Aerobic walking or strengthening exercise for osteoarthritis of the knee? A systemic review. Am Rheum Dis 2005 April;64(4):544-8 Wall R, Ross RP, Fitzgerald GF, Stanton C (2010). Fatty acids from fish: the anti-inflammatory potential of long-chain omega-3 fatty acid. Nutr Rev 68(5):280-9
5. Wall R, Ross RP, Fitzgerald GF, Stanton C (2010). Fatty acids from fish: the anti-inflammatory potential of long-chain omega-3 fatty acid. Nutr Rev 68(5):280-9
6. Ruggiero C, Lattanzio F, Gasperini B Andres-Lacueva C, Cherubini A (2009). Fatty acids from fish: the anti-inflammatory potential of long chain omega-3 fatty acids. Curr Pharm Des 15(36):4135-48.
7. Brouwer RW, Jakma TS, Verhagen AP, Verhaar JA, Bierma-Zeinstra SM. Braces and orthoses for treating osteoarthritis of the knee. Cochrane Database Syst Rev 2008:(1)
8. Felson DT, Mcalindon TE. Glucosamine and chondroitin for osteoarthritis: to recommend of not to recommend? Arthritis Care Res. 2000 Aug; 13(4):179-82.
9. Leeb BF, Schweitzer H, Montag K, Smolen JS. A meta-analysis of chondroitin sulfate in the treatment of osteoarthritis. J Rheumatol. 2000 Jan 27(1):205-11.
10. Richy F, Bruyere O, Ethgen O. Cucherat M, Henrotin Y, Reginster JY. Structural and symptomatic efficacy of glucosamine and chondroitin in knee osteoarthritis: a comprehensive meta-analysis. Arch Intern Med. 2003 Jul 14; 163(13):1514-22.
11. Poolsup N, Suthisisang C, Channark P, Kittikulth W. Clucosamine long term treatment and the progression of knee osteoarthritis: systemic review of randomized controlled trials. Ann Pharmacother 2005;39(6):1090-7.Epub 2005 Apr 26.
12. Bjordal JM, Klovning A, Ljunggren AE, Sloral L. Short term efficacy of pharmacotherapeutic interventions in osteoarthritic knee pain: A meta-analysis of randomized placebo-controlled trials. Eur J Pain 2007 Feb; 11(2):125-38.
13. Samson D.J., Grant M.D., Ratko T.A., Bonnell C.J., Ziegler K.M., Aronson N. Treatment of Primary and secondary osteoarthritis of the knee. Rockville, MD: Agency for Healthcare Research and Quality; 2007 Sep 1. Report No:157.
14. Laupattarakasem W, Laopaiboon M, Laupattarakasem P, Sumananont C. Arthroscopic debridement for knee osteoarthritis. Cochrane Database Syst Rev 2008;(1):CD005118.
15. Hubbard MJ. Articular debridement versus washout for degeneration of the medial femoral condyle. A 5-year study. J Bone Joint Surg Br 1996 March;78(2):217-9.
16. Dahl A, Toksvig-Larsen, Roos EM. A 2-year prospective study of patient-relevant outcome in patients operated on for knee osteoarthritis with tibial osteotomy. BMC musculoskeletal disord 2005;6-18.
17. Stukenborg-Colsman C, Wirth CJ, Lazovic D, WeferA. High tibial osteotomy versus unicompartmental joint replacement in unicompartmental knee joint osteoarthritis:7-10 years follow-up prospective randomized study. Knee 2001 October, 8(3):187-94.
18. Adili A, Bhandari M, Giffin R,Whately C, Kwok DC. Valgus high tibial osteotomy. Comparison between an Ilizarov and a Coventry wedge technique for the treatment of medial compartment osteoarthritis of the knee. Knee Surg Sports Traumatol Arthrosc 2002 May;10(3):169-76.
19. Coventry MB, Ilstrup DM, Wallrichs SL. Proximal tibial osteotomy. A critical long term study of 87 cases. J Bone Joint Surg Am. 1993;75:196-201.
20. Insall JN, Joseph DM, Msika C. High tibial osteotomy for varus gonarthrosis. A long term follow-up study. J Bone Joint Surg Am. 1984;66:1040-1048.
21. Engh,G.A., McAuley, J.P. Unicondylar arthroplasty: an option for high-demand patients with gonarthrosis. In Instructional Course Lectures, American Academy of Orthopaedics Surgeons. Vol 48, pp 143-148. Rosemont, Illinois, American Acedemy of Orthopaedic Surgeons, 1999.
22. Unicondylar knee arthroplasty in middle-aged patients: A minimum 5-year Follow-up. Philippe Cartier, Ahmed Khefacha, Jean-Louis Sanouiller, Keith Frederick. Orthopaedics 2007 August, Vol. 30, number 8.
23. Roberts VI, Esler CN, Harper WM. A 15-year follow-up study of 4606 primary total knee replacements. J Bone Joint Surg Br. 2007 Nov;89(11):1452-6
| Copyright ©2017 Asia Medical Specialists Limited. All rights reserved. |
