Biological Knee Replacement (BKR) FAQs
Biological Knee Replacement (BKR) FAQs
article written by Dr CC KONG
(Last updated on: Oct 13th 2020)
What is Biological Knee Replacement (BKR)?
Biological Knee Replacement (BKR) involves repairing a badly damaged knee with natural tissues instead of replacing the entire knee with a metal and plastic Total Knee Replacement (TKR).
Who needs BKR?
Young people with arthritis of their knees, who would otherwise need a total knee replacement. Total knee replacements work well, but they wear out, and need to be revised. Usually each revision is more difficult, and the results get worse each time, in a vicious cycle. Thus a total knee replacement is a good operation for a person in their sixties who wants to play a bit of golf, but an unfortunate proposition for a 30 or 40 year-old.
What is involved with a BKR?
Essentially repairing, reconstructing or replacing each structure that is broken in the knee. Exactly what is needed will vary between individuals. Typically there is ligament damage, often the anterior cruciate ligament (ACL), so an ACL reconstruction is performed. There is usually damage to the meniscal cartilage, so a meniscal repair, or, if the meniscus is absent or beyond repair, a meniscal transplantation is performed. The articular cartilage is almost always damaged, so one's own cartilage cells are grown in the laboratory and then replaced in the knee to grow new cartilage. Often the knee has become bowed, so the bone is cut and realigned to correct the loading. Usually all this requires two operations.
BKR: Stage I
Ligament Reconstruction
Any loose or torn ligaments are repaired or reconstructed. The most common ligament injury to the ACL. The ACL, in the middle of the knee, helps to control the complex bending and gliding motion of the knee. When the ACL is torn the joint loses its stability, leading to destruction of the articular and meniscal cartilage. ACL reconstruction restores the stability and reduces the likelihood of further degeneration. Usually we use ones own hamstring tendons to reconstruct the ACL (The tendons regrow). At the same time the whole knee joint is inspected arthroscopically, and, if the meniscal cartilage can be repaired, it is done at this time. If the articular cartilage is badly damaged, some cartilage cells are harvested and sent to the laboratory.
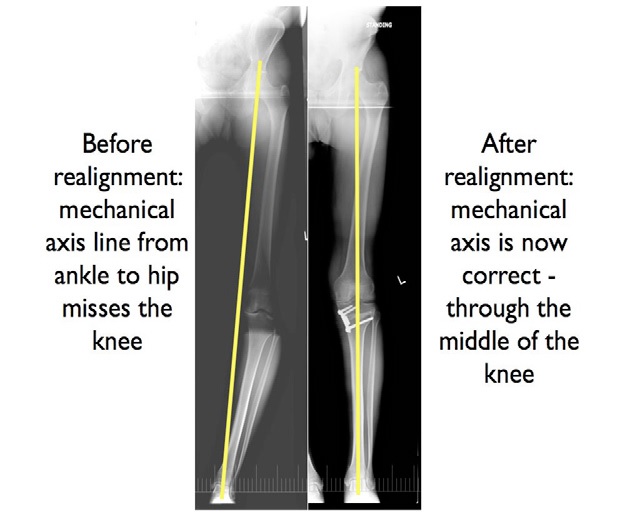
Alignment Correction
If the knee is bowed, the bone is cut to straighten it. It is fixed with a plate, and is strong enough to move the knee, but crutches are needed for about six weeks.
BKR: Stage II
Meniscus Replacement
The meniscal cartilage is the firm, fibrous shock absorber that rests in the knee between the femur and the tibia. If it is removed or damaged, the load on the articular cartilage increases, and it wears out ('Arthritis' usually means 'worn out articular cartilage'). Meniscus transplantation involves taking a meniscus from an organ donor and transplanting it to the patient. The donor is carefully screened for contamination, and if the contamination test results are clear, the tissue is provided to surgeons for transplantation. The menisci we use are provided by the Musculoskeletal Transplant Foundation in the USA and their record on contamination is
excellent. The operation is performed arthroscopically.
 |
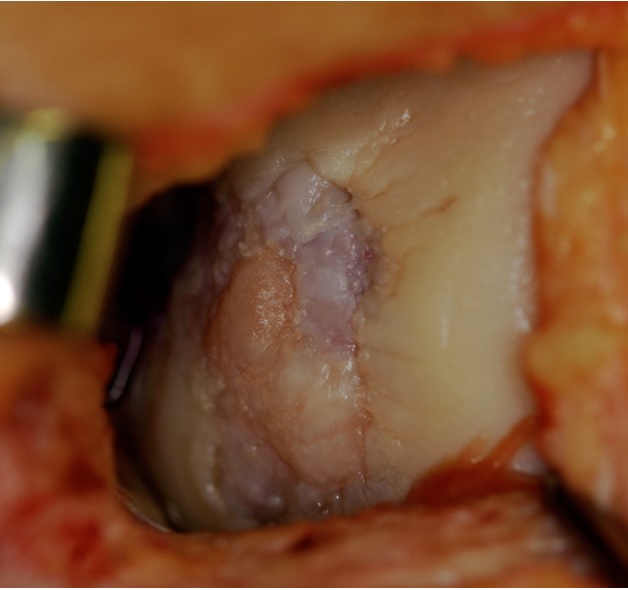
Articular Cartilage Replacement
Articular cartilage, once damaged, does not heal, which is why arthritis is such a huge problem. Autologous Chondrocyte Implantation heals cartilage by growing one’s own cells in the laboratory (which takes about 10 days) and then returning them to the knee. This is done by gluing the cells in place through a small incision. After the stage 2 operation one needs to use crutches for about 3 weeks.
Replacement Meniscus |

What about rehabilitation?
The rehabilitation process for BKR should begin prior to surgery, as patients need to be physically and mentally prepared for the operative procedure and the lengthy rehabilitation process. We call this 'prehabilitation'. Physiotherapy is required to build up the core muscle balance, lower limb flexibility and strength, and improve the gait. It speeds up the functional recovery and optimises the outcome of the operation. The physiotherapists follow a carefully designed protocol to try to get the most out of the knee, including, in some cases, return to sport. It takes about six months from the second operation to get back to light sports training, and the knee continues to improve for about 2 years.
 Damaged Articular Cartilage |
|
Should I take any supplements?
Cartilage supplement is part of the BKR programme. Glucosamine, a natural sugar made from chitin from the shells of shellfish is a key component of the extracellular matrix of articular cartilage. These sugars have charged side chains, which absorb water and provide lubrication and shock absorption for the articular cartilage that covers the ends of the bones in the joints. When people get degenerative arthritis, glucosamine and other sugars decline in concentration and lose some of their ability to absorb water. Glucosamine has been shown to be taken up in the cartilage and to improve the pain from arthritis as effectively as ibuprofen in gold standard 'double-blind prospective randomised controlled' trials.
That's quite an involved process – is it worth it?
If it saves one's knee and prevents or significantly delays the need for a total knee replacement, almost anything is worth it. At best, it could give one a near-normal knee, and allow one to play sport. The long-term results are not known, as BKR is a new procedure, but most of the various component procedures that make up the BKR have good results at up to ten years. In theory, the BKR should not 'wear out', because it really consists of returning the knee to its uninjured state and giving it a second chance, but if one were to develop arthritis in an un-injured 'good' knee, it is likely that it will also occur in the BKR.
| Copyright ©2017 Asia Medical Specialists Limited. All rights reserved. |
