Ankle Fracture FAQs
Ankle Fracture FAQs
written by Dr SW KONG
(Last updated on 6th May2024)
Summary
Ankle injuries are common. Sprains are best treated by physiotherapy. Severe sprains may benefit from about 10 days with a cast.(1) Minor (undisplaced) ankle fractures (breaks) can usually be treated with a cast/air-cast. More severe fractures require operation to fix the fractures. Recent studies have shown better outcomes if arthroscopy (keyhole surgery) is performed at the same time as the fracture operation to deal with cartilage injuries, which are not demonstrated on the X-rays.
Introduction
Ankle injuries are common. Many twisting injuries to the ankle result in sprains (i.e. torn ligaments). If the force is great enough, it may result in a fracture, (i.e. a broken bone) (Figs. 1 & 2). More information on sprains is in our Ankle Sprain FAQs.
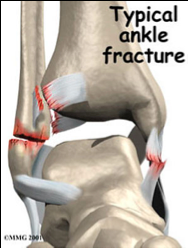 |  |  |
| Fig. 1 X-ray of a typical ankle fracture. The lateral malleolus (the tip of the smaller bone, called the fibula) is broken. | ||
Fig. 2 a and b: Diagram of the ankle fracture shown in the X-ray. In addition to the fracture seen on the X-ray, various ligaments are torn and there is cartilage damage where the bones have hinged against each other.
 Fig. 2a Beside fracture, there is widening of the joint space, which demonstrated the torn ligament as well |  Fig. 2b Besides fracture, there is loose fragment inside the ankle joint, which may causing cartilage damage if it is leave untreated Fig. 2b Besides fracture, there is loose fragment inside the ankle joint, which may causing cartilage damage if it is leave untreated |
My ankle hurts! Is it broken? Do I need an X-Ray?
When the ankle is sprained, it hurts a lot initially, but the pain usually gets better with ice and a support bandage. Although it will be painful, it is usually possible to walk. There is usually swelling and sometimes bruising, but the shape of the bones does not change.
With most fractures, the pain increases over the first few hours. Even light pressure on the bone causes severe pain and walking is usually impossible. If the fracture is displaced (ie the bones have moved out of position) the ankle is usually deformed as well as swollen and bruised (Fig. 3).
Minor fractures may be difficult to distinguish from severe sprains - if in doubt, ask your doctor to arrange an X-ray.
 Fig. 3 Typical bruising, swelling and deformity in a displaced ankle fracture |
Treatment
Ankle sprains
Ankle sprains are usually treated with rest, ice, compression, and elevation. A recent study suggested that the short-term recovery after a moderate to severe ankle sprain was better with a cast/aircast for about 10 days, but the long-term outcome was the same.(1-4) Physiotherapy, to help regain strength and balance, is important. More information is in the ‘Ankle Sprain FAQs’.
Ankle Fractures
Undisplaced fractures
If the bone is only ‘cracked’, with no displacement of the bones, wearing a cast is usually sufficient. If bone fragments are slightly displaced, it may be possible to ‘manipulate’ the bones into the right place (with the aid of a general anaesthetic) and hold them in place with a cast. The position of the bones has to be good – as little as 1mm displacement of the alignment between the tibia (the larger of the two shin bones) and the talus (in the foot) can increase pressure on the cartilage by 40% (8,9) potentially causing arthritis.
Displaced fractures
If the bones are significantly displaced, or manipulation fails to realign them sufficiently, open surgery is necessary; to fix the fragments into their correct alignment using screws and plates. Depending on the degree of bony damage, an aircast may be necessary following surgery, or if the fixation of the fracture is secure, your surgeon may prefer you to wear a normal sports shoe, so that ankle movement can begin as soon as possible.
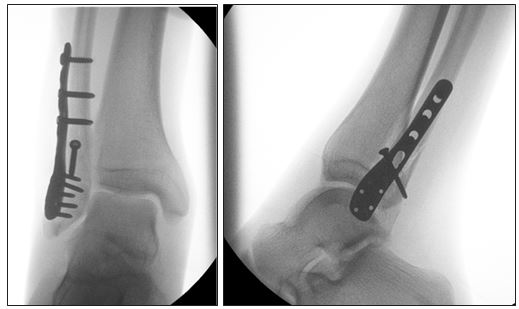 Fig. 4 (same patient as Fig. 1 with displaced fracture): |
Improved surgical outcomes with arthroscopic assisted/assessment during the ankle fracture fixation (1)
A study of arthroscopy (keyhole surgery) during ankle fracture fixation operation in 2002 (5) showed nearly twothirds of patients with ankle fractures also had cartilage injuries. Of these, over a quarter had bone or cartilage fragments loose inside the ankle joint. Loose pieces of bone or cartilage often cause further damage to the ankle joint. A simple ankle arthroscopy procedure can improve the outcome of the ankle fracture patients.
|
|
Fig. 5 Arthroscopy photograph shows a surgical instrument removing a loose piece of cartilage from the ankle joint. The cartilage is white. The pink tissue is inflamed joint lining. | |
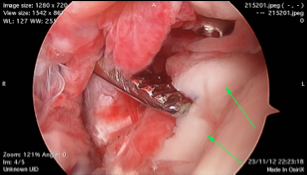
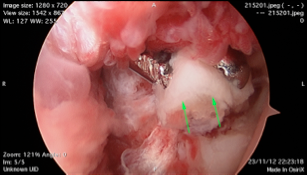
 Fig. 6 Arthroscopy photograph shows yellowish bone exposed where the white cartilage has been ripped off during the ankle injury. The instrument is a microfracture awl, which is used to make small holes in the exposed bone to encourage healing. |
Arthroscopic Management of Distal Tibio-fibular (Syndesmotic) Joint Injury (6,7)
Although X-ray is very accurate, it is slightly limited in diagnosing damage to the joint between the two shin bones, called the syndesmosis. The syndesmosis is important because it holds the talus bone of the ankle in the correct place, and as little as 1mm of talar displacement can increase joint load by 40%, (8,9) which will increase wear of the ankle joint.
Ankle arthroscopy has been proven to be more effective and accurate to diagnose syndesmotic injury than X-ray. (6, 7)
References
1. Cooke, M.W., et al., Treatment of severe ankle sprain: a pragmatic randomised controlled trial comparing the clinical effectiveness and cost-effectiveness of three types of mechanical ankle support with tubular bandage. The CAST trial. Health Technol Assess, 2009. 13(13): p. iii, ix-x, 1-121.
2. Hertel, J., Immobilisation for acute severe ankle sprain. Lancet, 2009. 373(9663): p. 524-6.
3. Kerkhoffs, G.M., et al., 10-day below-knee cast for management of severe ankle sprains. The Lancet, 2009. 373(9675): p. 1601.
4. Lamb, S.E., et al., 10-day below-knee cast for management of severe ankle sprains ? Authors’ reply. The Lancet, 2009. 373(9675): p.1602-1603.
5. Loren, G.J. and R.D. Ferkel, Arthroscopic assessment of occult intra-articular injury in acute ankle fractures. Arthroscopy, 2002. 18(4): p. 412-21.
6. Lui, T.H., K. Ip, and H.T. Chow, Comparison of radiologic and arthroscopic diagnoses of distal tibiofibular syndesmosis disruption in acute ankle fracture. Arthroscopy, 2005. 21(11): p. 1370.
7. Takao, M., et al., Arthroscopic diagnosis of tibiofibular syndesmosis disruption. Arthroscopy, 2001. 17(8): p. 836-43.
8. Ramsey PL. Changes in Tibiotalar area of contact caused by Lateral Talar Shift JBJS Am.1976; 58:356-357
9. Burns et.al Foot Ankle 1993;14:153-158
| Copyright ©2016 Asia Medical Specialists Limited. All rights reserved. |
