Rotator Cuff Tear FAQs
(Last update on: May 17th 2024)

What is the rotator cuff?
The rotator cuff is the joined-up of tendon of four of the muscles which move the shoulder, namely the subscapularis, supraspinatus, infraspinatus and teres minor. While most of the strength is supplied by the bigger muscles (deltoid, pectoralis major and lattissimus dorsi) the rotator cuff muscles control the stability and coordinated movement of the shoulder joint.
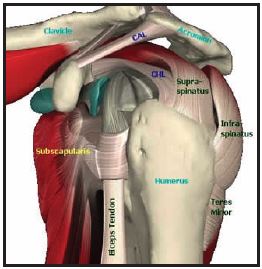 Rotator cuff tendons |
What is a rotator cuff tear?
Most rotator cuff injuries are common and increased with age. A rotator cuff injury is quite simply a tear of one or more of the rotator cuff tendons. Tears can vary hugely in severity from small partial thickness tears which may not cause any problems to massive full thickness tears which are difficult to treat. The longer a tear has been present, the weaker the shoulder and the larger the tear, the poorer the eventual outcome after treatment.
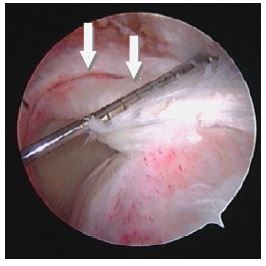 Arthroscopic view of a large rotator cuff tear, tear edge (arrow) |
What are the symptoms of rotator cuff tears?
The typical symptom of rotator cuff tears are:
- pain and weakness.
- The pain is usually diffuse.
- Lifting the arm above the shoulder will cause pain.
- Night pain is common.
- Weakness can range from mild weakness to being unable to lift the arm at all.
What is the natural history of rotator cuff tears?
A study which looked at asymptomatic tears by ultrasound showed that over 3 years, half of those who became symptomatic has the tears got larger, and no tears become smaller [1]. Another study showed about half of the patients with rotator cuff tear will have the tear enlarged in 5 years period, and 80% of them will develop symptoms [2]. Untreated tears eventually cause arthritis of the shoulder known as 'cuff tear arthropathy'. In conclusion, rotator cuff tears are at risk of progression and are likely to become symptomatic. Symptomatic tears usually get worse with time.
 MRI of rotator cuff tear. The arrow shows a gap in supraspinatus tendon. |
What are the treatment options for a rotator cuff tear?
Small partial thickness tears can commence non-operative treatment, and proceed to operation if non-operative treatment fails. All symptomatic complete rotator cuff tears should be repaired by operation, because the natural history is for the tear to become larger, and large tears can be very difficult to repair. However, non-operative treatment may be given for elderly patients who are not medically fit for an operation. A deep partial thickness tear behaves almost like a complete tear and should be treated with arthroscopic repair.
What is the non-operative treatment of rotator cuff tear?
- Anti-inflammatory drugs are used to reduce the pain.
- Physiotherapy, consisting of stretching exercises and strengthening exercises of the remaining rotator cuff muscles, helps to stretch out any capsule tightness to prevent the development of frank "frozen" shoulder and also helps to decrease impingement by stabilising the shoulder joint during movement. The exercises are quite subtle (more like ballet than weight-lifting) so need to be taught and supervised by a physiotherapist.
What is the operative treatment of a rotator cuff tear?
- Arthroscopic shoulder surgery is the mainstay of operative treatment for rotator cuff problems. It has been shown to provide results comparable to open surgery but without much of the associated morbidity. Unlike open surgery, there is no need to cut and split open the deltoid muscle, which may cause denervation and weaken this important mover of the shoulder. There is also less risk of scar and adhesion formation, which may compromise the repair. Other advantages include better scars, less post-operation pain and shorter hospital stays (most need just an overnight stay in hospital) and easier rehabilitation.
What does arthroscopic shoulder surgery involve?
It is a procedure performed under general anaesthesia in the operation room of the hospital. One lies on one’s side with the sore side up. The arm is held in a special traction device. Very small 'puncture' wounds are made to act as the portals for the arthroscope and the instruments. The joint is examined through an arthroscope connected to a video camera. Small instruments are placed through the portals to remove bone and soft tissue or to repair torn structures inside the joint. Although arthroscopic shoulder surgery is a technically demanding procedure which requires special equipment, training and experience, it offers an unsurpassed view of the inside of the shoulder joint that is not possible with open surgery. In addition, there is no need to damage anything to get into the shoulder joint.
Arthroscopic subacromial decompression is usually performed in patients with a rotator cuff tear as an adjunct procedure in rotator cuff repair to create more space for the cuff to glide through. With the arthroscope in the subacromial space between the undersurface of the acromion (process of the shoulder blade) and the rotator cuff, the hypertrophic (overgrown) structures causing impingement are removed by shaver, burr and electrocautery to create more space for the cuff. The hypertrophic bursal tissues and adhesions are removed. Then the undersurface of the acromion is scraped free of soft tissue. A few millimetres of bone are then removed from the undersurface of the anterior part of acromion together with any bony spurs to create a flat surface.
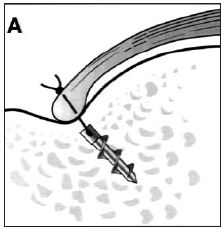
After performing the arthroscopic subacromial decompression, the torn tear of the cuff is minimally trimmed while the footprint of the cuff on the humeral head is freshened to allow better healing. The cuff is then mobilised by releasing any adhesions to allow repair with minimal tension. Then, depending on the configuration of the tear, a side-to-side repair can be performed using sutures, when there is a split in the substance of the tendon. To reattach the cuff back to the bone, a tendon-to-bone repair is required using special implants called “suture anchors”. Suture anchors are tiny screws with an eyelet through which pass one or two sutures. They are inserted into the bone under arthroscopic vision. The sutures are passed through the cuff tissue with special instruments. Knots are then tied inside the joint reattaching the tendons to bone. After the surgery, one is given a shoulder brace with a pillow holding the arm from the chest. This helps to relieve tension in the cuff repair. Usually one can leave the hospital the same or the next day.
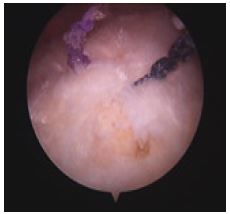
 Arthroscopic view after subacromial decompression |
Arthroscopic view after |
Suture anchor used to |
What about post-operative rehabilitation?
It is very important for one to follow a rehabilitation program after the surgery with the aim to protect the repair while allowing some motion to prevent the development of stiffness. One needs to wear a sling or shoulder brace for support and comfort after the procedure for 4 to 6 weeks, depending on the size of the tear. Range of motion exercises are followed by strengthening exercises, supervised by one’s physiotherapist. One can expect return to office and work on the computer table in one to two weeks, return to normal daily use of the arm (such as driving) after 2 months, and fully recover by 3-6 months, depending on the size of the tear.
The modern philosophy is to limit motion of the shoulder for the first 6 weeks to allow the cuff repair to heal, and accept that this will, almost inevitably, cause temporary stiffness of the shoulder. However, it is easier to deal with any stiffness than to deal with a failed cuff repair.
 Shoulder sling used after the surgery |
How successful is arthroscopic rotator cuff surgery?
Arthroscopic rotator cuff repair has been shown in numerous studies to yield 90% to 95% excellent to good results in terms of pain relief, patient satisfaction and improvement in function3-5. My personal series also showed that arthroscopic repair gave significant improvement in pain relief and functional outcome [6].
It is interesting to note that complete healing of the cuff repair is not always possible and, indeed, is not necessary to give good pain relief and patient satisfaction. This correlated well with the concept of "partial cuff closure" in massive rotator cuff tears as advocated by Dr Stephen Burkhart. Re-tear rates up to 30% have been reported following open repairs and arthroscopic repairs of a single tendon, but 85% of patients are still satisfied after the surgery [7].
However, for recovery of strength, the integrity of the cuff repair is more important. One study showed a correlation between a poor result and preoperative strength and active range of motion [8]. If patients had marked weakness or were unable to lift their shoulder beyond 100 degrees before the operation, there was an increased risk of a poor result. This is because patients who had poorer preoperative strength usually had larger cuff tears, which are harder to repair and to keep intact after surgery.
What’s new in arthroscopic rotator cuff repair?
The normal footprint of the supraspinatus tendon is 12mm in dimension from medial to lateral. Traditional single row repair does not fully restore the normal footprint. The newer technique of “double row repair” reproduces a larger footprint that improves the mechanical strength of the repaired tendons, improve healing of the repair, and lowers the rate of retear [9,10]. I find this technique effective.
 Double-row rotator cuff repair |
References
1. Yamaguchi K, Tetro AM, Blam O, Evanoff BA, Teefey SA, Middleton WD. Natural history of asymptomatic rotator cuff tears: a longitudinal analysis of asymptomatic tears detected sonographically. J Shoulder Elbow Surg. May-Jun 2001;10(3):199-203.
2. Tempelhof S, Rupp S, Seil R: Age-related prevalence of rotator cuff tears in asymptomatic shoulders. J Shoulder Elbow Surg 1999;8:296-299. 10471998
3. Burkhart SS, Danaceau SM, Pearce CE, Jr. Arthroscopic rotator cuff repair: Analysis of results by tear size and by repair technique-margin convergence versus direct tendon-to-bone repair. Arthroscopy. Nov-Dec 2001;17(9):905-912.
4. Murray TF, Jr., Lajtai G, Mileski RM, Snyder SJ. Arthroscopic repair of medium to large full-thickness rotator cuff tears: outcome at 2- to 6-year follow-up. J Shoulder Elbow Surg. Jan-Feb 2002;11(1):19-24.
5. Wolf EM, Pennington WT, Agrawal V. Arthroscopic rotator cuff repair: 4- to 10-year results. Arthroscopy. Jan 2004;20(1):5-12.
6. Chow KPB, LI W. Arthroscopic rotator cuff repair – Our experience and results. The 27th Hong Kong Orthopaedic Association Annual Congress, 2007.
7. Jost B, Pfirrmann CW, Gerber C, Switzerland Z. Clinical outcome after structural failure of rotator cuff repairs. J Bone Joint Surg Am. Mar 2000;82(3):304-314.
8. Ellman H, Hanker G, Bayer M. Repair of the rotator cuff. End-result study of factors influencing reconstruction. J Bone Joint Surg Am. Oct 1986;68(8):1136-1144
9. Lafosse L, Brzoska R, Toussaint B, Gobezie R. The Outcome and Structural Integrity of Arthroscopic Rotator Cuff Repair with Use of the Double-Row Suture Anchor Technique. Surgical Technique. J Bone Joint Surg Am 2008 90: 275-286.
10. Sugaya, Hiroyuki, Maeda, Kazuhiko, Matsuki, Keisuke, Moriishi, Joji. Repair Integrity and Functional Outcome After Arthroscopic Double-Row Rotator Cuff Repair. A Prospective Outcome Study. J Bone Joint Surg Am 2007 89: 953-960
Articles written/edited/reviewed by Doctors of Asia Medical Specialists ©2020 Asia Medical Specialists Limited. All rights reserved. |
