Carpal Tunnel Syndrome FAQ
Written By doctors of Asia Medical Specialists
(Last updated on: September 15th 2020)
Carpal Tunnel Syndrome FAQ
What is Carpal Tunnel Syndrome?
Carpal Tunnel Syndrome (CTS) is a condition due to compression of the median nerve as it travels through the wrist at the carpal tunnel. The main symptoms are pain, numbness, and tingling, in the thumb, index finger, middle finger, and the thumb side of the ring fingers. Symptoms typically start gradually and during the night. Pain may extend up the arm. Weak grip strength may occur and after a long period of time the muscles at the base of the thumb may waste away. In more than half of cases both sides are affected.
Anatomy of Carpal Tunnel
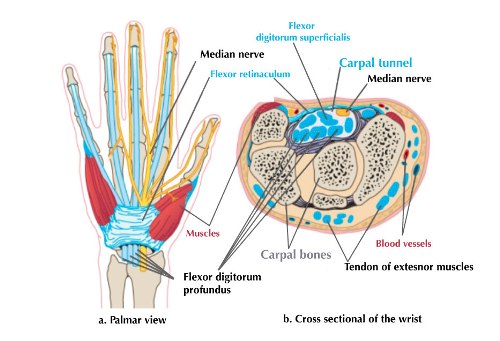
The carpal tunnel is a narrow passageway found on the anterior portion of the wrist covered by the superficial flexor retinaculum. It serves as the entrance to the palm for nine tendons surrounded by the synovial sheaths and the median nerve. The palmar cutaneous branch of the median nerve is given off prior to the carpal tunnel, travelling superficially to the flexor retinaculum.
What causes Carpel Tunnel syndrom (CTS)?
Pressure on the median nerve causes carpal tunnel syndrome. This pressure can come from swelling or anything that makes the carpal tunnel narrower.
There are a few causes for this swelling, including:
• Medical illnesses such as hypothyroidism, rheumatoid arthritis, and diabetes
• Repetitive movement of the wrist, especially if the wrist is bent down (your hands lower than your wrists)
• Pregnancy
• Infective tenosynovitis
• Idiopathic
There are a few causes resulted in narrow carpal tunnel
• Crystal deposition disease (gout)
• Trauma such as distal radius or wrist fracture
• Space-occupying lesion such as joint ganglion, nerve tumour
How is CTS diagnosed?
Your doctor will ask if you have any health problems, such as arthritis, hypothyroidism, diabetes, or if you are pregnant. He or she will ask if you recently hurt your wrist, arm, or neck. Your doctor will want to know about your daily routine and any recent activities that could have injured your wrist.
During the exam, your doctor will check the feeling, strength, and appearance of your neck, shoulders, arms, wrists, and hands. Your doctor may suggest tests, such as blood tests or electrodiagnostic tests.
Carpal tunnel syndrome-CTS treatment options?
Once the diagnosis confirmed, your doctor will start with nonsurgical treatment if the symptoms are mild, including:
- Stop activities that cause numbness and pain. Rest your wrist longer between activities.
- Try taking non-steroidal anti-inflammatory drugs (NSAIDs) to relieve pain and reduce swelling.
- Wear a wrist splint to keep the wrist at a neutral position at night. This takes pressure off your median nerve.
- Steroid injection may help to reduce the swelling from the flexor tendon sheath and other soft tissue inside the carpal tunnel to allow more space to the median nerve within days. 32 per cent of patients did not receive subsequent treatment after a single injection (4).
Surgery is the only option when there are muscle wasting and persistent symptoms not improve with the above treatments. It may take weeks to months to see the improvement. There is no fixed rule governing when the surgery should be performed. It highly depends on the severity of the symptoms, stage of the disease and risk factors. Elderly patients with longstanding disease, neurological deficits, and negative Phalen's test may not respond to surgery (2). The sooner you start treatment, the better your chances of stopping symptoms and preventing long-term damage to the nerve.
Surgery procedures - carpal tunnel release
There are 2 approaches to the carpal tunnel surgery to achieve decompression of the median nerve. If there is a mass (a nerve tumour, ganglion) inside the carpal tunnel, a conventional open approach is the best option. It is usually done under local anaesthesia or a combined monitored anaesthetic.
For the rest of the patients without any mass inside the carpal tunnel, the another approach is Endoscopic Carpal Tunnel Release (ECTR). It is proven to be as effective as conventional open surgery (5). This surgery is relatively minimally invasive.
Plase consult your doctor see which approach suits you.
Steps of the anaesthesia
(1) You will be lying on your back
(2) A tourniquet (a cuff similar for blood pressure measurement) applied on the arm required surgery to provide a bloodless field
(3) An IV access will be set up on the hand
(4) A local anaesthetic will be injected into the forearm via the IV access after tourniquet on
(5) You will feel numbness and loss of pain feeling starting from 5-10 mins after the injection and last for around 45 minutes
(6) Anaesthetist will give you some other sedatives to keep you calm and sleepy during the surgery
Steps of the surgery
(1) After cleaning the hand and arm with anti-septics
(2) Sterile drapes applied to cover you from elbow down to fingers
(3) You will feel the doctor touching you but without pain
(4) A 0.5-0.8cm transverse incision made on the wrist
(5) Canula will then be inserted into the carpal tunnel gently, and another 0.5-0.8cm incision will be made at the mid-palm for the cannula to exit
(6) An endoscopy will be inserted through the cannula to examine the tunnel
(7) After confirming the median nerve and flexor tendons, a small special knife passes into the tunnel to release the flexor retinaculum.
(8) The wrist incision will be closed with sutures
Postoperative care
Most of the patients with carpal tunnel release will be discharged on the same day. The surgical site is well covered with bulky outer dressing which should stay with you for the first few days. Splintage is usually not required. You will feel pain from the incision before you discharged because the local anaesthetic wears off. You should exercise your fingers within the bulky dressing. After the first few days, the outer dressing can then be removed. The wound is still covered with the thin layer of dressing till off stitches at day 12-14. You need to keep the dressing dry until you see your doctor. You will be provided with an oral painkiller to manage the surgical wound pain. Follow up in the office for wound check will be done in 1-2 weeks.
Expected discomfort during the recovery phase
Carpal tunnel release has split the transverse carpal ligament which will heal in 3-months time. Before the ligament healed, you will feel pillar pain (pain at the palm when you press on a hard surface), and weakness of hand grip. These problems will resolve by 3 months after the surgery.
Risk of surgery
Endoscopic or open carpal tunnel release carry a low risk of surgery. The overall complications rate is less than 1%. The wound infection rate is 0.32% (1). The remaining potential complications are rare, include an incomplete release of the transverse carpal ligament, palmar cutaneous branch of the median nerve, reflex sympathetic dystrophy, unsightly hypertrophic scar, superficial palmar arch, bowstringing of the flexor tendons and adherence of the flexor tendons (6).
The outcome of the surgery
One of the long-term follow-up studies showed that complete resolution of numbness was reported by 93.8% of patients, persistent numbness by 3.8%, and recurrent numbness by 2.5%. (3)
How can you keep carpal tunnel syndrome from coming back?
To keep carpal tunnel syndrome from coming back, take care of your basic health. Stay at a healthy weight. Don't smoke. Exercise to stay strong and flexible. If you have a long-term health problem, such as arthritis or diabetes, follow your doctor's advice for keeping your condition under control.
• You can also try to take good care of your wrists and hands:
• Try to avoid those activities in which your wrist has to be in an awful and prolonged flexion or extended position.
• Use your whole hand-not just your fingers-to hold objects.
• When you type, keep your wrists straight, with your hands a little higher than your wrists.
• Relax your shoulders when your arms are at your sides.
• If you can switch hands often when you repeat movements.
Media interview:
- ViuTV programme on Carpel Tunnel Syndrome - Chinese only (Dr Athena Au)
References
1. Werner BC, Teran VA, Deal DN.Patient-Related Risk Factors for Infection Following Open Carpal Tunnel Release: An Analysis of Over 450,000 Medicare Patients. Hand Surg Am. 2017 Oct 18. pii: S0363-5023(16)30628-1. doi: 10.1016/j.jhsa.2017.09.017.
2. Fakhouri F, Alsukhni RA, Altunbi B, Hawoot Z, Dabbagh R.Factors Correlated with Unfavorable Outcome after Carpal Tunnel Release Surgery. Asian J Neurosurg.2017 Oct-Dec;12(4):670-673. doi: 10.4103/ajns.AJNS_3_15.
3. Tang CQY, Lai SWH, Tay SC. Long-term outcome of carpal tunnel release surgery in patients with severe carpal tunnel syndrome. Bone Joint J.2017 Oct;99-B(10):1348-1353. doi: 10.1302/0301-620X.99B10.BJJ-2016-0587.R2
4. Evers S, Bryan AJ, Sanders TL, Gunderson T, Gelfman R, Amadio PC. Corticosteroid Injections for Carpal Tunnel Syndrome: Long-Term Follow-Up in a Population-Based Cohort.Plast Reconstr Surg. 2017 Aug;140(2):338-347. doi: 10.1097/PRS.0000000000003511.
5. GümüştaşSA, Ekmekçi B, Tosun HB, Bekler Hİ5. Similar effectiveness of the open versus endoscopic technique for carpal tunnel syndrome: a prospective randomized trial.Eur J Orthop Surg Traumatol. 2015 Dec;25(8):1253-60. doi: 10.1007/s00590-015-1696-0. Epub 2015 Aug 30.
6. MacDonald RI, Lichtman DM, Hanlon JJ, Wilson JN. Complications of surgical release for carpal tunnel syndrome. J Hand Surg Am. 1978 Jan;3(1):70-6.
Articles written/edited/reviewed by Doctors of Asia Medical Specialists ©2020 Asia Medical Specialists Limited. All rights reserved. |
