阿基里斯跟腱病常見問題
阿基里斯跟腱病常見問題
什麼是阿基里斯跟腱病?
「阿基里斯跟腱病」現在已被普遍理解為與阿基里斯跟腱疾病有關的疾病 (圖 1)。過去我們用的術語是肌腱炎,意味著發炎就是問題所在,但事實上這並不是炎症,而是退化問題 [1]。跟腱病可能是多種疾病過程的最終症狀。事實上到目前為止,此病尚未有一個被廣泛接受的病理證據,更遑論其治療方案。
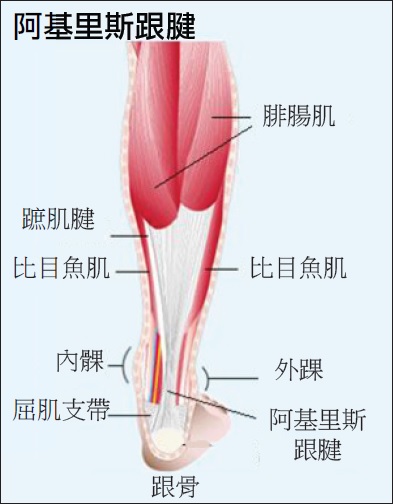 圖 1 阿基里斯跟腱及相關的腳部的結構 。 |
此文章所涉及的是非插入性阿基里斯跟腱病。
甚麼人會患上阿基里斯跟腱病?
無論是運動員或普羅大眾,都常有阿基里斯跟腱問題。這些問題會出現疼痛或腫脹,引致功能障礙。有時阿基里斯跟腱問題會引致其他足部及足踝問題,例如紅腫熱痛,甚至突然斷裂 (稱之為阿基里斯腱撕裂)。
有記錄顯示此病可與內在及外在的因素有關,但其關聯性並不容易被證實。
內在因素包括:年老、男性、系統性疾病、不良的血液供應、下肢排列不齊,和兩腿長度有異。外在因素包括:過度使用 (肌腱反覆承受大於生理可負擔的壓力) 、錯誤的訓練、局部或系統性使用類固醇,以及服用氟喹諾酮類的抗生素 [2]。阿基里斯跟腱病有可能是由內在和外在因素結合引致 [2]。有時候,患者的阿基里斯跟腱腫脹則與肌腱病變無關,如家族性高膽固醇血症患者的膽固醇有可能沉積於跟腱而引起腫脹。
如何診斷阿基里斯跟腱病?
病徵:患者通常投訴活動時感到疼痛,有時會有強烈的觸痛,或帶有紡綻狀的腫脹。主要透過臨床診斷來斷症,而磁力共振掃描(圖 2) 可更準確地勾畫受傷範圍、嚴重的疾病過程或撕裂程度。超聲波則是一個較廉宜的途徑來評估內肌腱病變過程 [3-5],且已經常在注射各種劑藥時,作為實時導引。
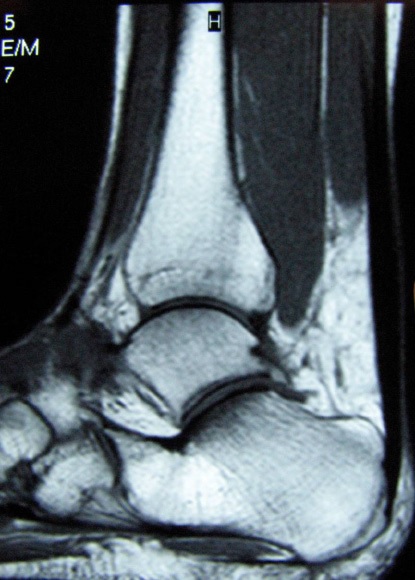 圖 2 磁力共振掃描檢查顯示的阿基里斯跟腱病。 |
有些病人很少有任何症狀,直至突然因為一個非生理的動作,導致急性引發慢性的斷裂 (圖 3)。大部分阿基里斯跟腱病的患者都有腓腸及比目魚肌 (小腿肌肉) 過緊的情況。
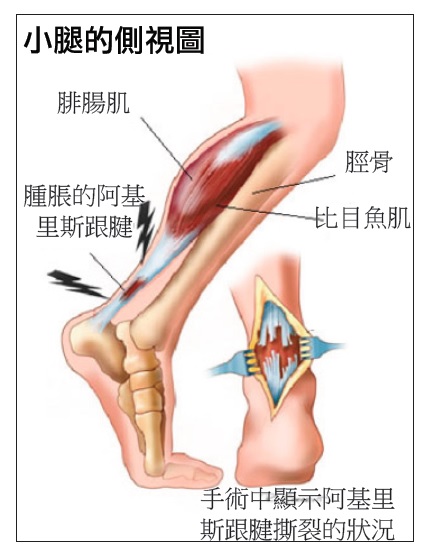 圖 3 破裂的阿基里斯跟腱 。 |
阿基里斯跟腱病會否導致阿基里斯跟腱斷裂?
通常不會。雖然我們認為阿基里斯跟腱斷裂的潛在成因是跟腱病,但通常「臨床癥狀不明顯」,即是無痛楚,所以患者察覺不到問題存在。一旦患者發現有阿基里斯跟腱病的「臨床癥狀」,即典型的痛楚和腫脹時,跟腱斷裂是不常見的。
如何治療阿基里斯跟腱病?
現時對此病的病原學、病理生理學及演化的理解有限,所以仍未有治療策略的共識。
多數的治療報告都局限於病例系列,只有不多的理據基礎。普遍來說,慢性阿基里斯跟腱病對保守療法的反應較差,與退化病過程中癒合能力差的組織學證據不謀而合 [6]。
目前有關以保守療法醫治阿基里斯跟腱病的文獻多屬回顧式,未經證實且缺乏證據。儘管如此,不論任何程度和階段的阿基里斯跟腱病,通常都鼓勵以非手術方法治療。
非手術治療策略包括調整活動,穿矯形鞋 (加入足跟墊及矯形器),以及物理治療尤其是離心練習,藉著壓迫跟腱及小腿肌肉來提高耐力和彈性。
有報告指出,非類固醇消炎藥物﹑體外衝擊波療法﹑及外用硝酸甘油酯,能減輕急性痛楚並對刺激癒合有正面作用。
雖然非類固醇消炎藥可紓緩急性痛症的症狀,但卻沒有證據顯示它們有助解決阿基里斯跟腱病。事實上,近年的文獻更顯示非類固醇消炎藥物有可能妨礙肌腱的癒合 [7]。
至於在跟腱內注射硬化劑或皮質類固醇,則有報告指出能為小部份患者幫助紓緩症狀 [8-10]。
高濃度血小板血漿:為患者注入自身的高濃度血小板血漿是很有效的治療方法。其原理是高濃度血小板能提供生長因子,促進肌腱癒合。這是一種安全且沒有副作用的治療,因為它只使用患者自身的血液。
動物研究中有組織學證據顯示肌腱的癒合,且癒合後的肌腱質素更佳 [11,12]。
亦有很多即將出版的文獻指出此療法對肌腱損傷,(包括阿基里斯跟腱、髕骨肌腱、膕繩肌腱、肩部二頭肌肌腱、網球和高爾夫球肘,及踝關節扭傷引致的急性韌帶損傷) 有很好的反應 [13]。
這醫療程序只需在診症室內進行。利用已消毒的注射器抽出 10 毫升血液,然後放入離心機 5 分鐘,血清會被隔離(圖 4),內含濃縮 10 倍的血小板(圖 5),在徒手或超聲波導引下,可直接注入病變的肌腱周圍。
|

康復需要 2 - 4 週的休息,令組織癒合。預期的臨床反應是痛楚得到改善。在大多數的報告中,患者只需接受一次注射,不過亦有部份患者需作重複注射。
雖然還未有高層次的証據(例如前瞻性隨機對照試驗) 或人體組織學資料,但臨床經驗對此療法有很不錯的評價。
強化小腿及伸展的離心練習:離心力強化練習報告 (圖 6),包括前瞻性及隨機研究,皆顯示這練習在大部份病人身上發揮滿意的效果 [14-18], 而且超聲波及磁力共振掃描証明肌腱厚度減少,並回復一個較生理性的外觀 [19,20]。但這個練習在運動員患者身上較非運動員患者有更好的成效 [21],故其功效仍需更多研究去証明。向心的負重 / 強化練習一直被視為會令已受損的肌腱惡化。
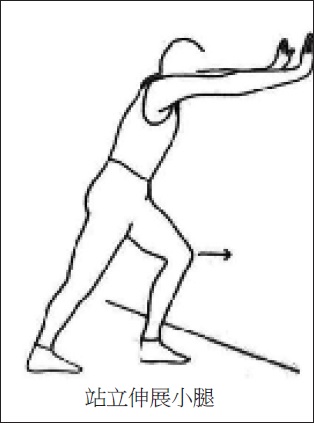 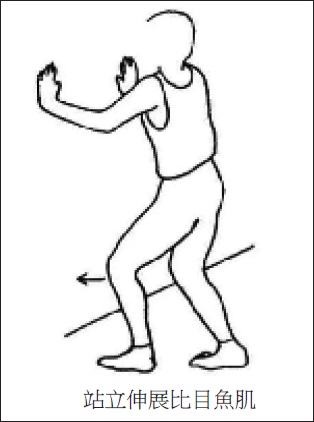 圖 6 離心伸展練習 。 |
手術治療:最近有文獻指出保守療法失敗的患者,有選用較進取的手術治療趨勢 [22-26]。手術的指標包括患者的年齡增長、病徵的持續時間延長、及阿基里斯跟腱病出現組織變異。雖然沒有一個公認的療法建議,但手術的選擇都是針對病理上的異常而度身訂定的。
嚴重的個案會有肌腱磨損,應以正統開放式的肌腱清創及增補術治療,有需要可用自體移植 [27,28]。中度或輕微的的個案常以簡單的開放式清創術治療 [23,29],或更少入侵性的療法,如經皮橫向肌腱切斷術 [25,30] 或內窺鏡清創術 [31] 治療。如果小腿肌肉攣縮限制腳背屈曲,近年提倡的療法,是延長肌腱 (例如施以 V - Y 型或 Z 型成型術) 或把小腿腓腸肌退縮再置 [32,33]。
參考文獻
1. Maffulli N; Kader D. Tendinopathy of tendo achilles Journal of Bone & Joint Surgery - British Volume 2002;84-1:1-8.
2. Kannus P. Etiology and pathophysiology of chronic tendon disorders in sports. Scandinavian Journal of Medicine & Science in Sports 1997;7-2:78-85.
3. Archambault JM, Wiley JP, Bray RC, Verhoef M, Wiseman DA, Elliott PD. Can sonography predict the outcome in patients with achillodynia? Journal of Clinical Ultrasound 1998;26-7:335-9.
4. Leung JL, Griffith JF. Sonography of chronic Achilles tendinopathy: a case-control study. Journal of Clinical Ultrasound 2008;36-1:27-32.
5. Peers KH, Brys PP, Lysens RJ, Peers KHE, Brys PPM, Lysens RJJ. Correlation between power Doppler ultrasonography and clinical severity in Achilles tendinopathy. International Orthopaedics 2003;27-3:180-3.
6. Vora AM, MS; Oliva, F; Maffulli, N. Tendinopathy of the main body of the Achilles Tendon Foot & Ankle Clinics 2005;10-2:293-308.
7. Li ZY, G; Khan, M; et al. Inflammatory response of human tendon fibroblasts to cyclic mechanical stretching. American Journal of Sports Medicine 2004;32-2:435-40.
8. Alfredson H, 2004. Preliminary results of colour Doppler-guided intratendi-nous glucocorticoid injection for Achilles tendonitis in five patients. Scand J Med Sci Sports 2004;14-4:269-70; author reply 70.
9. Koenig MJT-P, S; Qvistgaard, E; Terslev, L; Bliddal, H. Preliminary results of colour Doppler-guided intratendinous glucocorticoid injection for Achilles tendonitis in five patients. . Scand J Med Sci Sports 2004;14-2:100-6.
10. Alfredson HO, L. Increased intratendinous vascularity in the early period after sclerosing injection treatment in Achilles tendinosis: a healing response. Knee Surg Sports Traumatol Arthroscopy 2006;14-4:399-401.
11. de Mos M, van der Windt AE, Jahr H, van Schie HT, Weinans H, Verhaar JA, van Osch GJ. Can platelet-rich plasma enhance tendon repair? A cell culture study. American Journal of Sports Medicine 2008;36-6:1171-8.
12. Lyras DN, Kazakos K, Verettas D, Polychronidis A, Tryfonidis M, Botaitis S, Agrogiannis G, Simopoulos C, Kokka A, Patsouris E. The influence of platelet-rich plasma on angiogenesis during the early phase of tendon healing. Foot & Ankle International 2009;30- 11:1101-6.
13. Hall MP, Band PA, Meislin RJ, Jazrawi LM, Cardone DA. Platelet-rich plasma: current concepts and application in sports medicine. Journal of the American Academy of Orthopaedic Surgeons 2009;17-10:602-8.
14. Kingma JJ, de Knikker R, Wittink HM, Takken T. Eccentric overload training in patients with chronic Achilles tendinopathy: a systematic review. British Journal of Sports Medicine 2007;41-6:e3.
15. Knobloch K. Eccentric training in Achilles tendinopathy: is it harmful to tendon microcirculation? British Journal of Sports Medicine 2007;41-6:e2; discussion e.
16. Knobloch K, Kraemer R, Jagodzinski M, Zeichen J, Meller R, Vogt PM. Eccentric training decreases paratendon capillary blood flow and preserves paratendon oxygen saturation in chronic achilles tendinopathy. Journal of Orthopaedic & Sports Physical Therapy 2007;37-5:269-76.
17. Petersen W, Welp R, Rosenbaum D. Chronic Achilles tendinopathy: a prospective randomized study comparing the therapeutic effect of eccentric training, the AirHeel brace, and a combination of both. American Journal of Sports Medicine 2007;35-10:1659-67.
18. Woodley BN-W, R. J; Baxter, GD. Chronic Tendinopathy : effectiveness of eccentric exercise British Journal of Sports Medicine 2006.
19. Shalabi A. Magnetic resonance imaging in chronic Achilles tendinopathy. Acta Radiol Suppl (Stockholm) 2004-432:1-45.
20. Ohberg LA. 12(5): 465 – 70, 2004. . Effects on neovascularisation behind the good results with eccentric training in chronic midportion Achilles tendinosis. Knee Surg Sports Traumatol Arthroscopy 2004;12-5:465-70.
21. Sayana MM, N. Eccentric calfs muscle training in non-athletic patients with Achilles tendinopathy. Journal of Science Medicine Sport 2006.
22. Green DR, Ruch JA, McGlamry ED. Correction of equinus-related forefoot deformities: a case report. Journal of the American Podiatry Association 1976;66-10:768-80.
23. Scott AT, Le IL, Easley ME. Surgical strategies: noninsertional Achilles tendinopathy. Foot & Ankle International 2008;29-7:759-71.
24. Tallon C, Coleman BD, Khan KM, Maffulli N. Outcome of surgery for chronic Achilles tendinopathy. A critical review. American Journal of Sports Medicine 2001;29-3:315-20.
25. Testa V, Capasso G, Benazzo F, Maffulli N. Management of Achilles tendinopathy by ultrasound-guided percutaneous tenotomy. Medicine & Science in Sports & Exercise 2002;34-4:573-80.
26. Aaron T. Scott; Ian L. D. Le MEE. Surgical Strategies: Noninsertional Achilles Tendinopathy. Foot & Ankle International 2008;20-6:759-71.
27. Coull RF, R; Stephens, MM. Flexor hallucis longus tendon transfer: evaluation of postoperative morbidity. Foot & Ankle International 2003;24-12:931-4.
28. Wilcox DB, DR; Anderson, JG. Treatment of chronic achilles tendon disorders with flexor hallucis longus tendon transfer/augmentation. Foot & Ankle International 2000;21-12:1004-10.
29. Maffulli NB, PM; Moore, D; King, JB. Surgical decompression of chronic central core lesions of the Achilles tendon. American Journal of Sports Medicine 1999;27-6:747-52.
30. Maffulli N, Testa V, Capasso G, Bifulco G, Binfield PM. Results of percutaneous longitudinal tenotomy for Achilles tendinopathy in middle- and long-distance runners. American Journal of Sports Medicine 1997;25-6:835-40.
31. Maquirriain J, Ayerza M, Costa-Paz M, Muscolo D. Endoscopic surgery in chronic achilles tendinopathies: A preliminary report. Arthroscopy 2002;18-3:298-303.
32. Costa ML, Donell ST, Tucker K. The long-term outcome of tendon lengthening for chronic Achilles tendon pain. Foot & Ankle International 2006;27-9:672-6.
33. Gentchos CE, Bohay DR, Anderson JG. Gastrocnemius recession as treatment for refractory achilles tendinopathy: a case report. Foot & Ankle International 2008;29-6:620-3.
34. Laborde JM. Neuropathic plantar forefoot ulcers treated with tendon lengthenings. Foot & Ankle International 2008;29-4:378-84.
35. Maluf KS, Mueller MJ, Strube MJ, Engsberg JR, Johnson JE. Tendon Achilles lengthening for the treatment of neuropathic ulcers causes a temporary reduction in forefoot pressure associated with changes in plantar flexor power rather than ankle motion during gait. Journal of Biomechanics 2004; 37-6:897-906.
此文章原文由亞洲專科醫生以英文撰寫 © 2017 亞洲專科醫生有限公司,版權所有 |
